Ya en el año 98 Frankel Sherman postulaba que dosis de finasteride tan bajas como 0.05 mg/día, podían inhibir el 60/70 % de la DHT en cuero cabelludo. Es una interesante y deseable teoría, pero en nuestra experiencia con pacientes medicados hemos visto que algunos pueden estabilizar con dosis menores a 1 mg, pero no todos, la dosis es personal y no podemos generalizar. Aún así en casos determinados (efectos secundarios, edad madura, poca área a preservar, miedo o respeto al fármaco, etc..) se puede probar con dosis menores con la idea de disminuir los niveles de DHT a un nivel donde no hayan efectos secundarios y ralenticemos en lo posible la evolución de la alopecia. Nos gusta decir que medicación no es blanco o negro, sino que hay muchos grises en el medio y ese gris es personal para cada uno.
gracias.
Sherman Frankel, April 6, 1998
Recently, the Food and Drug Administration (FDA) approved the use of the drug PROSCAR, under a new name, PROPECIA, for treatment of male pattern baldness. The medical term for the drug is finasteride but it is marketed under these two different names. The PROSCAR pill is 5 milligrams while the PROPECIA pill is 1 milligram (mg). PROSCAR is intended for older men suffering from benign prostatic hyperplasia, (BPH). It is not surprising that PROSCAR would affect hair growth since it inhibits the normal conversion of testosterone to dihydrotestosterone. It is well known that hair growth and impotence are connected to levels of dihydrotestosterone.
In the last few years it has been claimed that PROSCAR is ineffective in the treatment of BPH, both from studies of the medical literature (1), and in a more recent double blind study.(2). However there is a claim that for men with very large prostates, the incidence of choice of surgery is smaller and there is improvement in urinary retention.(3)
The double blind studies of PROPECIA do not extend beyond a few years, yet the predominant users are expected to be males in their thirties. The drug must be continued indefinitely if the new hair growth is to continue over one's lifetime.
With the announcement of the new use of PROSCAR, we recently used the Freedom of Information Act to obtain the documentation leading to the approval by the Food and Drug Administration for the use of PROPECIA.
We have examined the material and come to the conclusions that occupy the remainder of this note. The questions we address relate to dosages, side effects, and other conclusions to be drawn from the double-blind studies presented by Merck to the FDA.
A key question that needs resolution is the size of the dose of the main ingredient, finasteride, that should be used. In the PROSCAR studies it was found that, in measurements of prostate shrinkage, a 1 mg dose could not be distinguished from a 5mg dose. Yet the dosage recommended by Merck for PROSCAR was 5 mg and the effect of dosages lower than 1 mg were not studied. In the PROPECIA studies, the effects of a range of dosages were reported to the FDA. These studies examined how the drug inhibited the conversion of testosterone to dihydrotestosterone which is the significant feature affecting hair growth. This inhibition was observed to be 60-70 % in the (NDA 20-788) Merck study.
A significant result deals with the depletion of dihydrotestosterone (THD)and enhancement of testosterone (T), as measured in the scalp skin as a function of dosage.
Figure:
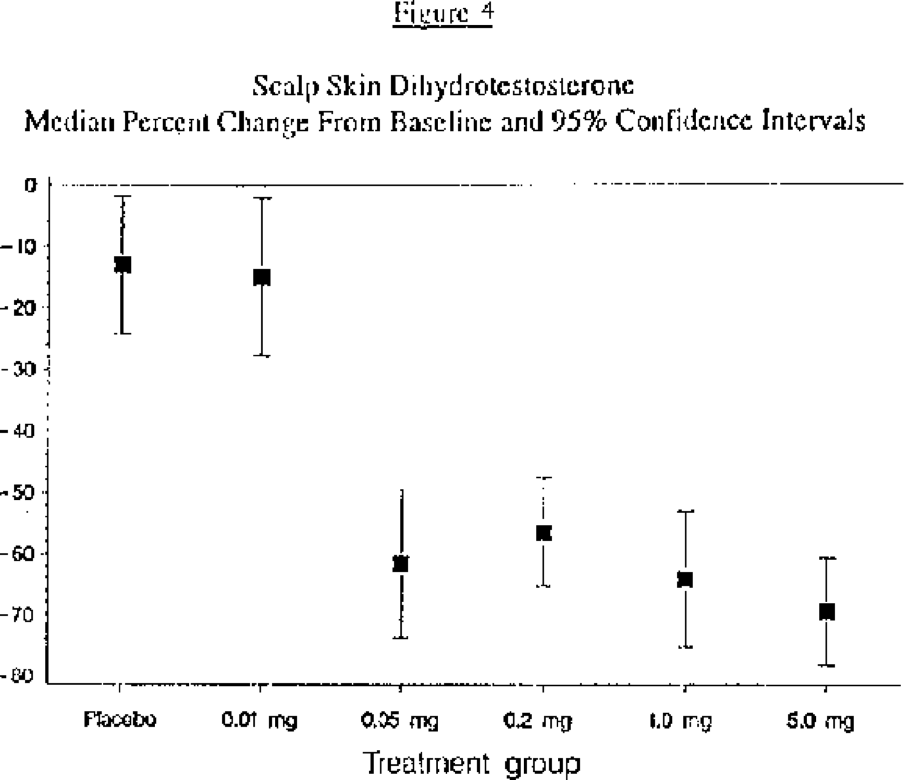
As seen in Fig. 1, reproduced from the FDA material, the percent change of DHT for placebo and .01 mg finasteride were identical and essentially zero within a reasonable statistical estimate. The change dropped by 60 % for a .05 mg dose and stayed that way for all dosages up to 5 mg. Thus a 20 times smaller dose than PROPECIA had the same effect on the DHT.
Figure:
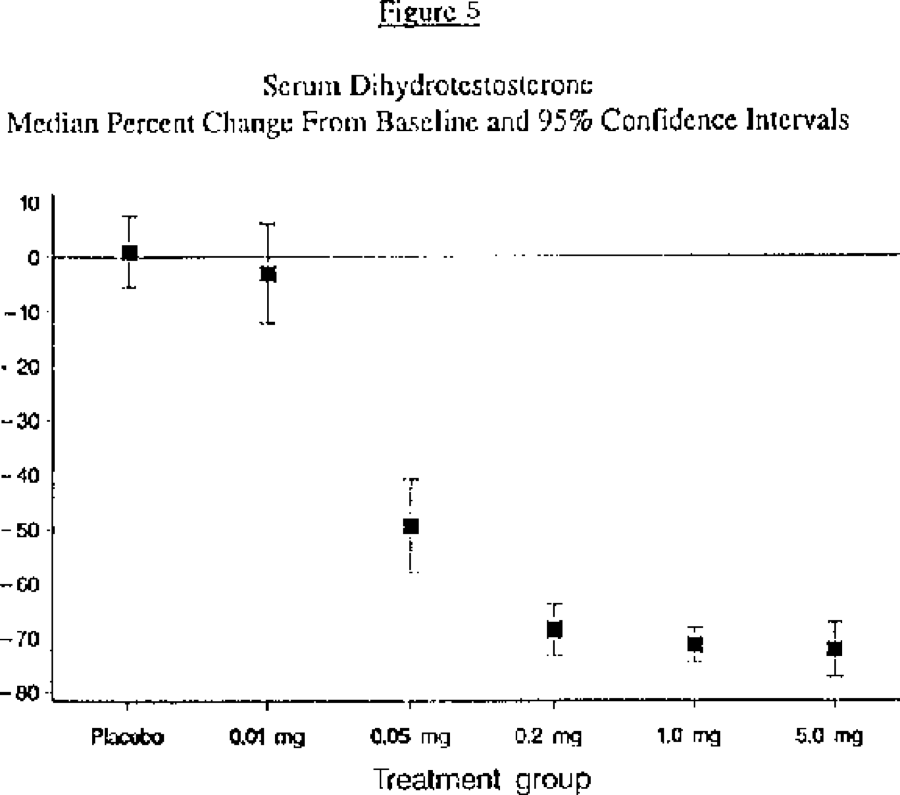
A similar dose dependence was seen for the serum DHT (Fig. 2) where the effect was independent of dose above 0.2 milligrams.
Figure:
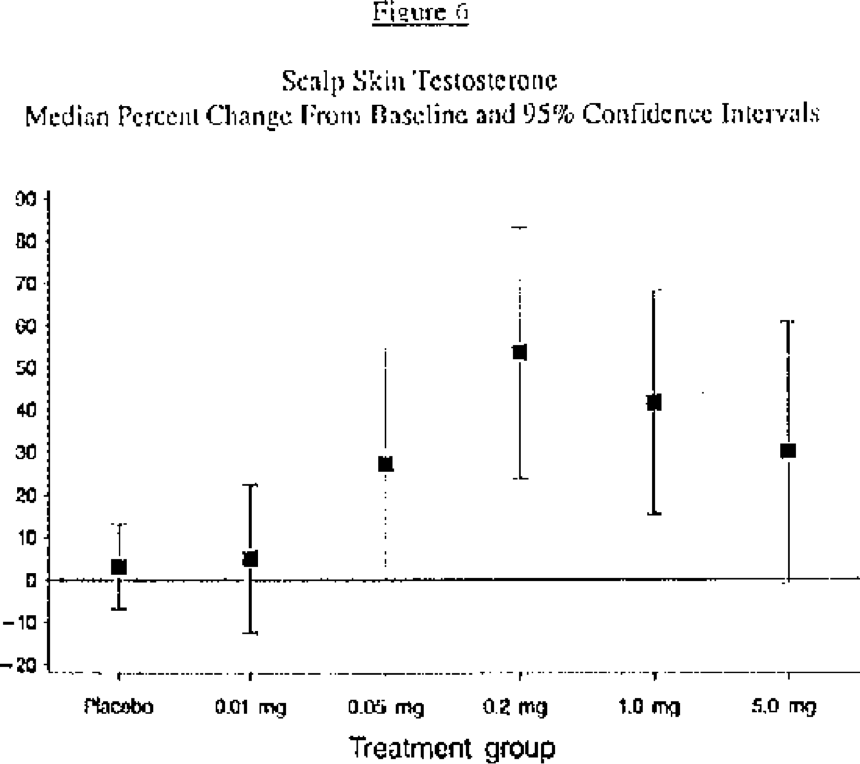
The dose dependence appears also in the accompanying rise in T, one-onehundredth the 5 mg dose being identical in its effect on the scalp skin testosterone. See Fig. 3.
Typically, the price of 5 mg PROSCAR is $76 for 30 pills, a months supply. For 1 mg PROPECIA it is $54. Therefore a PROPECIA user would pay only $15 if he were to cut up the 5 mg pills. However the above depletion studies suggest that a dosage of 0.2 mgs would be as effective as the 1 mg dose, bringing the price down to $3. For the user willing to dissolve the PROSCAR pill, (it is soluble in ethanol), or divide it up by other means, the monthly cost would be seventy-six cents.
The data supplied to the FDA on ``efficacy parameters'', (NDA 20-788, table 8.1.2.4.2) compared .2 and 1.0 mg dosages in hair count, investigator assessment, and global photographic assessment but did not present data for other dosages above .02 mg. However the sample of participants (100) was small and the differences between the .2 and 1.0 dosages in the first two cases were not apparent and, in the photographic assessment, which showed a larger mean improvement for 1 mg, the values overlapped statistically at the 95% confidence level.
We now turn to the question of side effects. One set of such effects is sometimes called ``sexual adverse events''. Three of these are impotence, libido decrease, and ejaculation disorder. We have examined the results of Trials 1-5 (047,081,087,089,092), submitted by Merck to the FDA. These are studies carried out over about a year. What the data show is that about 2% of such users show these adverse events, with about 1% resulting in impotence and about 1/2 percent each showing libido decrease or ejaculation disorder. Breast enlargement and sensitivity are also occasionally reported. Merck has presented no data answering the question of whether the several effects are correlated, i.e., if one suffers impotence is one also likely to have the other side effects as well. Yet a potential user might want an answer to this question before committing to the drug.
More seriously missing are data that trace the growth, if any, in these side effects over long periods. These side effects seem to disappear after discontinuance of the drug after a short period of usage but there are no data on longtime usage.
The reduction in the ejaculate volume, more important to young users than the elderly users suffering from BPH, clearly affects the fertility of users with already low ejaculate volume, possibly dropping the quantity below the needed fertility level. While average reductions in volume are reported there are no reported data on the liklihood of large reductions.
From the earlier studies on PROSCAR, it was observed that the prostate size was decreased, falling off and appearing to level out near year's end. But the accuracy was too low to predict whether or not, over a longer period like a decade, the prostate continues to shrink. However an extension of the study for two more years showed a further decrease in prostate size with a 5 mg dose, again with no definite plateauing effect. It is not known whether this decrease will continue over time or whether it will present a problem.
Another effect is related to the PSA score which is often used as a possible test for the onset of prostate cancer. PROPECIA produces a decrease in the PSA score. Merck states that the average observed decease is 50%. Publishing average decreases is not sufficient without presenting some indication of the spread of such decreases. Such a decrease could mask the increase in score for a patient showing signs of cancer and might inhibit the request for a biopsy. It is feared that dermatologists might not transfer PROPECIA usage information to the patient's urologist and because of fluctuations, "doubling the PSA level", the recommended guideline, would be misleading.
Conclusions:
The FDA has approved a drug for which there are no long term studies that relate to sexually adverse effects, and their correlations, a drug that must be taken for a lifetime by young men who wish to retain their hair. (Of course, the knowledgable user can decide for himself whether he wishes to take the negative risks, but there are no warnings in the drug insert that only longer term tests can predict the probabilities and severity of the various adverse side effects and that the potential user should take this into consideration.)
The data on the dosage dependence of the depression of conversion to DHT, reproduced in this report from the material obtained under the FOIA, does not appear in the medical literature or in the drug insert. Thus the fact that the dosage has been set by the manufacturer at a level far larger than the level measured as necessary for the main function, has not been reported publicly. Yet, the vastly lower dosages, reported in the data submitted to the FDA, would be expected to reduce the chance of side effects.
Unfortunately, nothing is found in the FDA reviews of the request for approval of PROPECIA, commenting on the renarkable dosage data reproduced in this note.






























